Hall ticket no. 1601006126
This is an online e logbook to discuss our patients deidentified health data shared after taking her/guardian's signed informed consent
Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs
This E log also reflects my patient centre’s online learning portfolio and valuable inputs on the comment box is welcome.
Case Presentation of Upper motor neuron lesion who is also a known case of diabetes and hypertension.
A 50 years old female, from Suryapet who is a homemaker was brought to the OP as she was unable to lift her left arm and left leg. and her mouth was deviated to right side since 3 days.
History of Presenting Illness-
The patient was apparently asymptomatic 7 days ago, then she felt dizzy for a brief period of time.
3 days ago, she felt weakness during morning hours in her left arm while making breakfast and noticed weakness in her left leg followed by fall on the floor.
Weakness was sudden in onset and rapidly progressed to a state where she was unable to move her left side of the body.
There were no similar attacks in the past.
There was no history of headache, nausea, vomiting, fever or burning micturition and she is not a known case of migraine.
No sensory impairment, no dysphagia, no giddiness, no tinnitus, no hearing impairment, no visual disturbance, no bowel and bladder incontinence and no new gait abnormality
Past medical history-
She is a known case of diabetes mellitus since 5years and Hypertension since 3 years for which she was on medication.
Glimipramide 0.2mg
Voglibose 0.2mg and
tenegliptin 20mg
Metformin 500mg
Telmesartan 40mg
Amlodipine 125mg.
She is not a known case of Tuberculosis, bronchial asthma, thyroid disorders, epilepsy.
Menstrual history
She had undergone hysterectomy 4 years ago for fibroid uterus
Family history:- No significant history.
Personal history
she has mixed diet
Normal appetite.
Bladder habits are regular.
bowel movements are irregular.
she has not been able to pass stools since 5 days.
No allergic reactions to any known drugs
General Examination:-
The patient was conscious cooperative oriented to the time place and person and cooperative lying on the bed in supine position.
Patient was afebrile
Pulse = 69 beats per minute.
- Blood pressure = 140/70 mm of Hg.
- Respiratory rate = 16 cycles per minute.
- JVP is not elevated
- There is NO Pallor, Icterus, Clubbing, Cyanosis, Generalized lymphadenopathy and Edema.
Nervous system examination
the patient is conscious, alert, oriented and cooperative.
Higher mental function is intact and presence of slurring of speech.
Right handedness
Cranium and spine- no abnormalities detected.
Signs of meningeal irritation- neck rigidity, Kernig's, Brudzinski are negative
there is no kinking or bruits in carotid arteries.
Cranial nerves examination:-
Pupils- left and right reactive to light
3rd, 4th, 6th no abnormalities
5th nerve- sensory- normal
- motor- jaw jerk +ve
7th nerve- mouth deviation towards- right
Drooling of contents of food from left side
frowning present
-absent nasolabial folds on left side
-blowing and whistling absent

Taste sensation on anterior 2/3rd of tongue present
Corneal reflex present on both sides
Vestibulocochlear nerve- Rinnes Weber, Schwabach test normal on both sides
9th, 10th, 11th- gag reflex +


Motor function-
Nutrition- normal- no wasting seen on both sides
Tone- right upper limb- normal
Right lower limb- normal
Left upper limb- normal
Left lower limb- normal
Power- right upper limb- 5/5
Right lower limb- 5/5
Left upper limb- 0/5
Left lower limb- 0/5
Reflexes:- Right left
i) Superficial Reflexes
. Corneal reflex present present
. Conjunctival reflex present present
. Plantar reflex flexor extensor
ii) Deep Reflexes
Right left
Biceps +2 +3
Triceps +2 +3
Supinator + 2 +3
Knee +2 +3
Ankle. Not elicited
Plantar flexor Extensor
Sensory system
Superficial -fine touch,temperature, pain -present
Deep-position, vibration, crude touch, stereognosis, 2point discrimination- present
Cerebellum- Speech, nystagmus, tremors- absent
Coordination
Finger nose test ,finger finger test,heel knee test-present
Cardiovascular system- S1 and S2 heard no murmurs, not a known case of valvular heart disease atrial fibrillation
Respiratory system- Bilateral air entry present
Respiratory-Normal vesicular breath sounds,bilateral air entry present
GIT -no significant findings
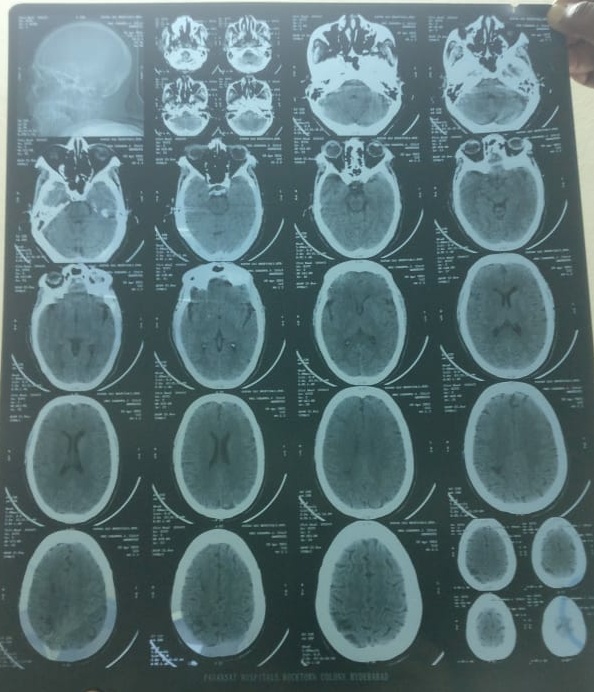
Provisional Diagnosis-
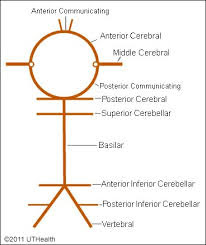
Left Sided hemiparesis with left UMN type of facial paresis (due to right middle cerebral artery infarct)
Medical Management-
Aspirin 75mg
Clopidogrel 75mg
Pantoprazole 40mg
Atorvastatin 40 mg
Physiotherapy
GRBS monitoring 8th hourly.

No comments:
Post a Comment