A 50yr old female was presented in casualty with giddiness, double vision and slurred speech
50yrs old female, homemaker from nalgonda with following history-
8yrs she had 2-3 episodes of staring look, not reapong to commands, which lasted for 5-10 minutes, when taken to the hospital she was told to be hypertensive and stated her on anti hypersensitives. no imagong was done during that period .
6 yrs ago she had menorrhagia (? fibroid) amd underwent hysterectomy.
post operative period her sutures were not healing as expected under evaluation she was found to be diabetic and started her on oral Hypoglycemic agents glimipramide bd
10days ago when she was cleaning the floor she slipped on wet floor and had a blunt trauma on ybe left side of abdomen
she complained of pain in the left hypochondrium and was taken to a local RMP and is on painkillers since then
since a day she again complained of pain in the left hypochondrium that was not subsiding then she was again taken to local doctor, while lying in the bed to get nsaid inj 10 min later she felt that her tongue was swollen and was unable to speak
After going home they noticed her speach was slurred, she also complained of giddiness which aggrevated on sitting up, swaying while walking and diplopia was sudden in onset.
Patient attributed all her complaints against i.m injection but her attenders thought there could be more than just a reaction to an injection so they bought her to casualty.
No c/o of weakness, tingling or numbness of limbs
no c/o of headache, loss of consciousness, head trauma, seizures or altered sensorium.
no c/o of havkng any difficulty in chewing, swallowing or deviation of mouth.
she is able to turn on the bed on her own and she can feel her own clothes
no complaints suggesting bowel and bladder, she was able yo feel fullness of her bladder.
she has regular bowel and bladder habits.
no history of chest pain, palpitations, sob, facial puff, pedal edema.
she is a k/c/o HTN since 10yrs and is on medication- atenolol 50mg and amlodepine 5mg
she is a k/c/o DM since 6 yrs and is on medication(OHA)
is is not a k/c/o Bronchial asthma, tuberculosis, epilepsy, CAD
o/e
pt is c/c/c
afebrile in touch
PR-111
BP 140/80
RR 18
GRBS- high
SPO2- 96
she has no pallor, icterus, cyanosis, clubbing, lymphadenopathy or pedal edema
CVS- S1 S2+
RS- central trachea, BAE+ NVBS
PA- soft, tender present in the left hypochondrium
CNS- oriented to time,place,person
memory : recent, remote intact
speech: slurred,
no dysarthria.
cranial nerves:
1-intact
2: diplopia in binocular vision
monocular vision:normal
colour vision:normal
3,4,6- normal(extra occular movements)
5-normal( muscles of mastication+sensations of face)
7- Loss of nasolabial fold to on right
8- didnt elicit
9,10,11,12-normal
motor- tone -normal
power 5/5 in b/l lowerlimbs 5/5 in upper limbs
reflexes :biceps:b/l:2+
triceps, supinator, knee were absent, plantars: mute initially later when elicited-
triceps- +2
supinator+2,
knee and ankle absent
Plantars upgoing, right and left mute
sensory: crude ,pain,temp, fine touch, joint position, proprioception are normal in all dermatomes
cerebellum-
finger nose- normal
Finger finger test normal
Heel knee to test normal
no dysdidokinesia.
rhomberg's- swaying with eyes open
nystagmus+, Nystagmus to right and vertical gaze nystagmus+
gaze evoked , horizontal more on right gaze with fast component towards the right
Gait: slow paced, wide based, swaying on both sides
stride: regular with path deviation
turns: normal
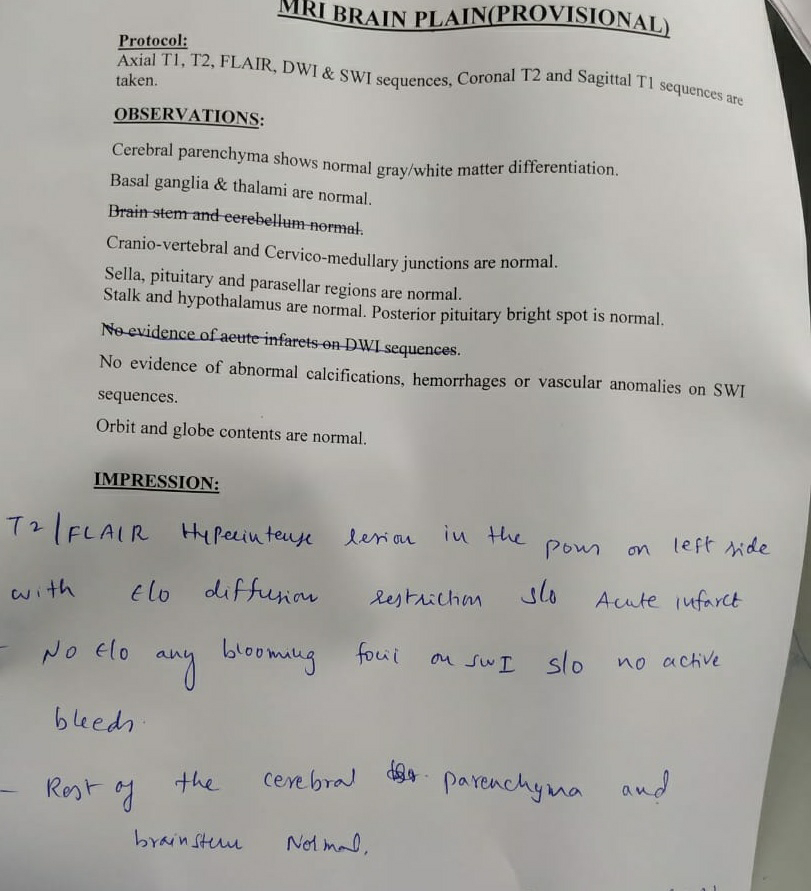
provisional diagnosis- Acute ischaemia cva with infarct in left pons
with uncontrolled dm2
with hypertension
treatment-
ivf NS l, RL continuous infusion
insulin- HAI 16 units stat
inj h actrapid infusion at 6ml/hr
inj pan 4p mg iv od
inj avil 1 aml iv sos
tab atenolol- amlodepine 50/5 po od





Soap notes
ICU BED 6-
50/F

S- c/o giddiness, on walking.
double vision decreased compared to presentation.
slurring of speech+
O- pt is c/c/c
Afebrile
PR-84/min
Bp-130/80mmhg
Cvs:S1,S2+
R.S: bae+nvbs
p/a:soft, nt
CNS: oriented to time,place,person
memory : recent, remote intact
speech: slurred,
naming, repetition,comprehension+
cranial nerves: 1-intact
2: visual acuity, colour vision:normal
monocular vision:normal
colour vision:normal
3,4,6-
eyelids-no ptosis
eyeballs at rest-normal
extraocular movements-normal b/l
pupillary light reflex-direct and indirect-normal
binocular horizontal diplopia.
5-normal
7-normal
8- didnt elicit
9,10,11,12-normal-no dysphagia,dysarthria.
motor- tone -normal
power 4-/5 in b/l lowerlimbs 5/5 in upper limbs
reflexes :biceps:b/l:2+
triceps:2+
supinator+
knee:2+
plantars:b/l flexor
sensory: crude ,pain,temp
fine touch
joint position
proprioception
normal in all dermatomes
not able to perform rhomberg's (as shes swaying even with eyes open)
cerebellum- no finger nose/finger finger incordination
no rebound, dysdidokinesia.
nystagmus+,gaze evoked , horizontal more on right gaze with fast component towards the right
vertical upbeat and downbeat +
Gait: slow paced, swaying on both sides
stride:regular with path deviation
turns: normal
total insulin requirement from 20/11 to 21/11
including infusion and basal bolus regimen
72 units
inj nph 20---*---20
inj regular- 10---*---8
A- Acute ischaemia cva with infarct in left pons
with uncontrolled dm2
wih hypertension
P- inj nph-20IU(8am---8pm)
inj hai 10---10---8IU(8am---2pm---8pm)
tab ecosprin 150mg/od
tab atorvas 20mg /od
tab clopidogrel 75mg od
7 point profile







No comments:
Post a Comment